
女性脱发(专业版)
女性脱发通常是指体内雄激素过高等内分泌失调引起的脱发。脱发是指头发脱落的现象,为头发正常生长周期的一部分。
其他名称:女性头发薄
英文名称:Alopecia in Women,Hair Thin in Women,
最常见的雄激素性脱发原因:女性脱发可能由毛囊对双氢睾酮(DHT)的敏感性引起;此外,绝经后雌激素水平下降,也可能有助于脱发。结果导致毛囊逐渐萎缩,以及缩短了头发生长周期,新生头发越来越少。
造成脱发的主要因素可包括如下:
调整饮食与生活方式
营养与草本综合干预
以下是基于循证医学和循证营养学有关文献综合的结果。
有助于防控女性脱发的营养和草药补充剂,主要包括如下:
1.维生素D:
越来越多的证据表明,维生素D参与头发周期的调节1-3。在一个由210名女性型脱发女性组成的案例系列中,超过60%的女性维生素D水平低于正常水平4。血清维生素D水平低与包括斑秃在内的自身免疫性疾病有关5,6。休止期脱发与维生素D缺乏有关7,而维生素D水平低与休止期脱发和女性型脱发女性的脱发程度更高有关8。
在一项为期12周的试验中,48名轻度至中度斑秃患者每天接受二次含有钙泊三醇(维生素D合成形式)的局部溶液治疗。试验结束时,超过62%的参与者的头发再生率达到75%或更好,27%的参与者的发质再生率达到100%9。一名7岁男孩患有斑秃的案例也令人信服:在对局部米诺地尔加氢化可的松没有反应后,该男孩在局部钙泊三醇治疗三个月后经历了完全的头发再生10。一项针对20名斑秃儿童和34名健康对照的研究发现,维生素D水平与脱发严重程度评分呈负相关—随着维生素D水平的升高,脱发严重程度评分下降11。
动物和临床前模型表明,局部使用维生素D和钙泊三醇可能有助于预防化疗诱导的脱发,一些证据表明这种治疗可以促进头发再生12-14。在一项研究中,局部维生素D显著减少了雌性小鼠化疗引起的脱发15。
2.维生素B族:
46名患有弥漫性脱发的妇女每天口服维生素B5 (泛酸)200mg,每天肌肉注射维生素B6,持续20-30天。6个月后重复治疗,结果改善了头发状况,减少了脱发16。动物研究结果表明,维生素B6与L-胱氨酸结合,可防止化疗药物阿霉素引起的脱发17,18。
严重的生物素(维生素B7)缺乏可能是某些基因突变的结果,导致脱发以及其他一些严重的健康问题19。在一项研究中,38%自我报告脱发的女性表现出生物素缺乏症20。在狗身上,补充生物素可能有助于促进毛发生长21,但人类临床试验尚未证实这一发现。一些初步证据表明,补充生物素可能有助于治疗由丙戊酸药物引起的脱发22。
3.角蛋白:
蛋白质缺乏是脱发的一个公认原因,角蛋白是头发的主要成分和主要结构元素。角蛋白合成的年龄相关下降可能导致发干的稳定性和柔韧性恶化23,24。这可能会使头发在梳洗、使用造型产品和工具时容易干燥和断裂。
在一项研究中,在50名有头发紧张或受损迹象的女性中,将一种含有新型可溶性角蛋白(Cynatine®)加维生素和矿物质的补充剂与安慰剂进行了比较。Cynatine含有一种经过特殊处理的、高度生物利用的角蛋白肽形式,是半胱氨酸的丰富来源。90天后,Cynatine配方组的脱发减少,头发强度增加,改善了生长期、休止期和生长期与休止期比率;与安慰剂相比,头发外观更好25。
4.硅:
硅是一种存在于体内的微量元素,被认为是头发的结构成分26。硅化合物在许多可食用植物中很常见27。两项研究着眼于补充提供硅的原硅酸对头发健康的影响。
在一项研究中,50名女性每天服用10mg原硅酸或安慰剂,持续20周。研究结束时,接受硅补充剂的女性头发脆性降低28。在第二项研究中,48名头发细的女性接受了相同的化合物或安慰剂治疗9个月;与安慰剂相比,补充组的头发强度和弹性得到了更好的保留,头发厚度增加29。
5.锌:
锌缺乏与脱发有关30,31。锌在正常毛囊活动、防止毛囊退化和促进毛囊恢复方面发挥着重要作用31。此外,锌可以作为抗雄激素和5-α还原酶的调节剂32。
研究发现,患有雄激素性脱发、休止期脱发和斑秃的男性和女性的血清锌水平都低于没有脱发的人31。早期研究表明,使用锌补充剂纠正相关休止期脱发患者的锌缺乏可以改善脱发33。
斑秃患者锌水平较低与严重程度增加、持续时间延长和治疗耐药性可能性增加有关34,35。在一项非对照临床研究中,15名患有斑秃和低锌水平(≤70mcg/dL)的受试者每天接受50mg葡萄糖酸锌治疗。12周后,9名受试者的头发再生,与锌状况改善相关36。此外,病例报告表明,在接受紫外线加锌治疗的斑秃患者中,持续补充葡萄糖酸锌可能有助于保持头发恢复37。
6.铁:
缺铁会导致休止期脱发38-40。在女性型脱发41,42、休止期脱发42,43和绝经前脱发44的女性中观察到铁蛋白(一种铁储存蛋白)水平较低。一项研究发现,最低的铁蛋白水平与最严重的脱发有关。可以考虑对脱发女性进行铁状况评估,并在必要时补充铁42。
7.必需脂肪酸:
一项针对120名早期脱发女性的试验发现,与对照组相比,六个月内每天补充460mg鱼油、460mg黑加仑籽油(提供γ-亚麻酸GLA)、1mg番茄红素和少量维生素E和维生素C可以改善头发密度。与安慰剂组相比,补充组的生长期头发更多,休止期头发更少45。
在一项啮齿动物研究中,大多数服用DHA(来自鱼油的二十二碳六烯酸)的动物都能免受化疗诱导的脱发的影响46。在另一项针对6只脱发恒河猴的研究中,每天用ω-3(72mg)和ω-6(26mg)脂肪酸治疗与脱发减少有关47。几项研究发现,将DHA与紫杉醇(一种常用的化疗药物)结合,可以减少该药物的毒副作用,包括脱发48-50。
8.生育三烯酚:
生育三烯酚是维生素E家族的成员,天然存在于大麦、小麦胚芽以及某些类型的谷物和坚果中51。与更常见的维生素E形式生育酚类似,有四种生育三烯酚标记为α、β、γ和δ51,52。生育三烯酚被认为具有重要的维生素E活性,特别是在抗炎、降低胆固醇和辐射防护方面52,53。
新出现的证据表明,生育三烯酚可能有助于促进头发健康。在一项涉及38名患有不同类型和程度脱发的女性和男性的研究中,接受23IUα-生育酚加50mg混合生育三烯醇补充剂的患者在八个月内头发数量增加了34%以上,而接受安慰剂的患者头发数量略有减少54。
9.硒:
硒的摄入对健康的毛囊功能很重要,硒缺乏可能在脱发中发挥作用55,56。在一项针对64名多囊卵巢综合征女性的为期八周的随机对照试验中,32名女性每天补充200mcg硒,另一半女性则服用安慰剂。试验结束时,与安慰剂相比,硒组的脱发显著减少57。
10.锯棕榈:
锯棕榈被广泛用于治疗前列腺肥大和雄激素性脱发58。一项针对26名23-64岁、患有轻至中度雄激素性脱发男性的随机对照试验发现,200mg锯棕榈提取物、50mg β-谷甾醇以及补充量的卵磷脂、胆碱、肌醇、烟酸和生物素的组合,对头发生长和质量测量是有效的。对头发生长和外观满意度的自我评估,以及研究者对头发密度的评估都显著改善59。
一项针对50名20至50岁雄激素性脱发男性的非对照研究发现,局部使用锯棕榈会增加头发数量60。另一项试验对100名轻度至中度雄激素性脱发患者进行了为期两年的每日320mg锯叶棕榈提取物和每日1mg非那雄胺的疗效比较。非那雄胺使68%的受试者的头发再生,而锯棕榈组中38%的受试人的头发生长得到改善;锯棕榈的治疗耐受性良好61。研究人员认为,锯棕榈抑制5-α还原酶的能力至少是其积极作用的部分原因58;一些人提出,将锯棕榈或β-谷甾醇与肉碱和α-硫辛酸等抗炎剂结合可能会增强其有效性62,63。
11.绿茶:
有证据表明,绿茶及其主要多酚表没食子儿茶素没食子酸盐(EGCG)可能有助于防止脱发和帮助头发再生。在一项小鼠研究中,局部EGCG溶液可防止睾酮诱导的脱发64。在一项针对自发性脱发小鼠的研究中,添加到饮用水中的绿茶多酚溶液促进了头发的生长,而不是用白开水促进头发的生长65。EGCG在实验室环境中以及在人类受试者中刺激真皮乳头细胞并促进人类毛囊中的毛发生长66。
12.甲磺酰甲烷(MSM):
一种天然含硫有机物质,具有抗氧化、抗炎、抗皮肤衰老和促进头发生长等多种生物功能67,68。动物研究表明,饮食中补充0.2%的MSM可以改善小猫的毛发质量68。
13.褪黑素(外用):
褪黑激素可能有助于脱发的局部治疗。虽然还不知道褪黑素是如何对抗脱发的,但它对抗氧化应激的能力,被认为在脱发中起着重要作用69,以及它刺激毛囊生长的能力已经被提出70。
在一项早期对照试验中,40名患有女性脱发或弥漫性脱发的女性每晚在头部涂抹1毫升0.1%的局部褪黑素溶液或安慰剂溶液。六个月后,局部褪黑素组在生长期的头发明显增多71。
一组针对早期雄激素性脱发男性和女性的四项研究评估了褪黑素与其他外用药物联合治疗脱发的效果。在第一项研究中,将同样含有生物素和银杏叶提取物的0.0033%褪黑素溶液每晚涂抹在30名男性和女性的头皮上,持续90天。研究人员和参与者都报告说,脱发的严重程度在第30天有所下降,在第90天有了更大的改善。在第二项研究中,35名男性在六个月内每晚使用相同的溶液。研究人员注意到,三个月后头发数量和密度平均增加了29%,六个月后数量和密度分别增加了近43%和41%,超过50%的参与者对治疗有反应。第三项研究使用了毛发计数测试,参与者计算每天早上梳头60秒时脱落的毛发数量,作为衡量反应的指标。在为期90天的试验中,20名女性参与者的脱发数量有所下降,但使用褪黑素溶液的40名男性参与者的脱发量没有下降。最后一项研究包括901名男性和990名女性,他们每晚使用该溶液。拔毛测试显示,经过90天的治疗,近62%的参与者没有脱发,近23%的参与者有新的头发生长。此外,褪黑素溶液治疗似乎可以改善患有这种头皮疾病的参与者的脂溢(红色、发痒、鳞状皮肤)70。
更多内容可点击其个性化综合干预方案如下:
以及参阅本网如下专文了解更多:
医疗干预
如果脱发由疾病引起,通过治疗、身体康复后头发会重新长出。
医生可能推荐如下治疗措施:
有助于预防一些脱发的措施包括如下:
参考文献:
1. Amor KT et al. Does D matter? The role of vitamin D in hair disorders and hair follicle cycling. Dermatology online journal. 2010;16(2):3.
2. Malloy PJ et al. The role of vitamin D receptor mutations in the development of alopecia. Molecular and cellular endocrinology. Dec 5 2011;347(1-2):90-96.
3. Aoi N et al. 1alpha,25-dihydroxyvitamin D3 modulates the hair-inductive capacity of dermal papilla cells: therapeutic potential for hair regeneration. Stem cells translational medicine. Aug 2012;1(8):615-626.
4. Siah TW et al. Female Pattern Hair Loss: A Retrospective Study in a Tertiary Referral Center. International journal of trichology. Apr-Jun 2016;8(2):57-61.
5. Mahamid M et al. Association between vitamin D levels and alopecia areata. The Israel Medical Association journal: IMAJ. Jun 2014;16(6):367-370.
6. Aksu Cerman A et al. Vitamin D deficiency in alopecia areata. Br J Dermatol. Jun 2014;170(6):1299-1304.
7. Cheung EJ et al. Vitamin and Mineral Deficiencies in Patients With Telogen Effluvium: A Retrospective Cross-Sectional Study. Journal of drugs in dermatology. Oct 01 2016;15(10):1235-1237.
8. Rasheed H et al. Serum ferritin and vitamin d in female hair loss: do they play a role? Skin Pharmacol Physiol. 2013;26(2):101-107.
9. Cerman AA et al. Topical Calcipotriol Therapy for Mild-to-Moderate Alopecia Areata: A Retrospective Study. J Drugs Dermatol. Jun 2015;14(6):616-620.
10. Kim DH et al. Successful treatment of alopecia areata with topical calcipotriol. Annals of dermatology. Aug 2012;24(3):341-344.
11. Unal M et al. Serum vitamin D level is related to disease severity in pediatric alopecia areata. Journal of cosmetic dermatology. Apr 26 2017.
12. Jimenez JJ et al. Protection from chemotherapy-induced alopecia by 1,25-dihydroxyvitamin D3. Cancer research. Sep 15 1992;52(18):5123-5125.
13. Schilli MB et al. Reduction of intrafollicular apoptosis in chemotherapy-induced alopecia by topical calcitriol-analogs. The Journal of investigative dermatology. Oct 1998;111(4):598-604.
14. Wang J et al. Protection against chemotherapy-induced alopecia. Pharmaceutical research. Nov 2006;23(11):2505-2514.
15. Chen G et al. Protection against cyclophosphamide-induced alopecia and inhibition of mammary tumor growth by topical 1,25-dihydroxyvitamin D3 in mice. International journal of cancer. Jan 19 1998;75(2):303-309.
16. Brzezinska-Wcislo L. [Evaluation of vitamin B6 and calcium pantothenate effectiveness on hair growth from clinical and trichographic aspects for treatment of diffuse alopecia in women]. Wiadomosci lekarskie (Warsaw, Poland: 1960). 2001;54(1-2):11-18.
17. D'Agostini F et al. Chemoprevention of doxorubicin-induced alopecia in mice by dietary administration of L-cystine and vitamin B6. Archives of dermatological research. Jan 2013;305(1):25-34.
18. D'Agostini F et al Chemoprevention of smoke-induced alopecia in mice by oral administration of L-cystine and vitamin B6. J Dermatol Sci. Jun 2007;46(3):189-198.
19. Zempleni J et al. Biotin and biotinidase deficiency. Expert review of endocrinology & metabolism. 2008;3(6):715-724.
20. Trueb RM. Serum Biotin Levels in Women Complaining of Hair Loss. International journal of trichology. Apr-Jun 2016;8(2):73-77.
21. Frigg M et al. Clinical study on the effect of biotin on skin conditions in dogs. Schweizer Archiv fur Tierheilkunde. 1989;131(10):621-625.
22. Famenini S et al. Evidence for supplemental treatments in androgenetic alopecia. J Drugs Dermatol. Jul 2014;13(7):809-812.
23. Giesen M et al. Ageing processes influence keratin and KAP expression in human hair follicles. Experimental dermatology. Sep 2011;20(9):759-761.
24. Mubki T et al. Evaluation and diagnosis of the hair loss patient: part II. Trichoscopic and laboratory evaluations. Journal of the American Academy of Dermatology. Sep 2014b;71(3):431.e431-431.e411.
25. Beer C et al. A clinical trial to investigate the effect of Cynatine HNS on hair and nail parameters. TheScientificWorldJournal. 2014;2014:641723.
26. Martin KR. Silicon: the health benefits of a metalloid. Metal ions in life sciences. 2013;13:451-473.
27. Jurkic LM et al. Biological and therapeutic effects of ortho-silicic acid and some ortho-silicic acid-releasing compounds: New perspectives for therapy. Nutrition & metabolism. 2013;10(1):2.
28. Barel A et al. Effect of oral intake of choline-stabilized orthosilicic acid on skin, nails and hair in women with photodamaged skin. Archives of dermatological research. Oct 2005;297(4):147-153.
29. Wickett RR et al. Effect of oral intake of choline-stabilized orthosilicic acid on hair tensile strength and morphology in women with fine hair. Archives of dermatological research. Dec 2007;299(10):499-505.
30. Saper RB et al. Zinc: an essential micronutrient. American family physician. May 1 2009;79(9):768-772.
31. Kil MS et al. Analysis of serum zinc and copper concentrations in hair loss. Annals of dermatology. Nov 2013;25(4):405-409.
32. Gupta M et al. Zinc therapy in dermatology: a review. Dermatol Res Pract. 2014;2014:709152.
33. Karashima T et al. Oral zinc therapy for zinc deficiency-related telogen effluvium. Dermatologic therapy. Mar-Apr 2012;25(2):210-213.
34. Abdel Fattah NS et al. Evaluation of serum zinc level in patients with newly diagnosed and resistant alopecia areata. Int J Dermatol. Jan 2016;55(1):24-29.
35. Bhat YJ et al. Trace element levels in alopecia areata. Indian journal of dermatology, venereology and leprology. Jan-Feb 2009;75(1):29-31.
36. Park H et al. The therapeutic effect and the changed serum zinc level after zinc supplementation in alopecia areata patients who had a low serum zinc level. Annals of dermatology. May 2009;21(2):142-146.
37. Lux-Battistelli C. Combination therapy with zinc gluconate and PUVA for alopecia areata totalis: an adjunctive but crucial role of zinc supplementation. Dermatologic therapy. Jul-Aug 2015;28(4):235-238.
38. Grover C et al. Telogen effluvium. Indian journal of dermatology, venereology and leprology. Sep-Oct 2013;79(5):591-603.
39. Levy LL et al. Female pattern alopecia: current perspectives. International journal of women's health. 2013;5:541-556.
40. Malkud S. Telogen Effluvium: A Review. Journal of clinical and diagnostic research: JCDR. Sep 2015;9(9):We01-03.
41. Park SY et al. Iron plays a certain role in patterned hair loss. J Korean Med Sci. Jun 2013;28(6):934-938.
42. Rasheed H et al. Serum ferritin and vitamin d in female hair loss: do they play a role? Skin Pharmacol Physiol. 2013;26(2):101-107.
43. Moeinvaziri M et al. Iron status in diffuse telogen hair loss among women. Acta dermatovenerologica Croatica: ADC. 2009;17(4):279-284.
44. Deloche C et al. Low iron stores: a risk factor for excessive hair loss in non-menopausal women. European journal of dermatology: EJD. Nov-Dec 2007;17(6):507-512.
45. Le Floc'h C et al. Effect of a nutritional supplement on hair loss in women. Journal of cosmetic dermatology. Mar 2015;14(1):76-82.
46. Takahata K et al. Protection from chemotherapy-induced alopecia by docosahexaenoic acid. Lipids. 1999;34 Suppl:S105.
47. Hamel AF et al. Fatty acid supplements improve hair coat condition in rhesus macaques. Journal of medical primatology. 2017 Oct;46(5):248-251.
48. Bradley MO et al. Tumor targeting by conjugation of DHA to paclitaxel. Journal of controlled release: official journal of the Controlled Release Society. Jul 6 2001;74(1-3):233-236.
49. Wolff AC et al. Phase I study of docosahexaenoic acid-paclitaxel: a taxane-fatty acid conjugate with a unique pharmacology and toxicity profile. Clinical cancer research. Sep 1 2003;9(10 Pt 1):3589-3597.
50. Harries M et al. Phase I/II study of DHA-paclitaxel in combination with carboplatin in patients with advanced malignant solid tumours. British journal of cancer. Nov 1 2004;91(9):1651-1655.
51. Ahsan H et al. A review of characterization of tocotrienols from plant oils and foods. J Chem Biol. 2015;8(2):45-59.
52. Peh HY et al. Vitamin E therapy beyond cancer: Tocopherol versus tocotrienol. Pharmacol Ther. 2016;162:152-169.
53. Jiang Q. Natural forms of vitamin E: metabolism, antioxidant, and anti-inflammatory activities and their role in disease prevention and therapy. Free Radic Biol Med. 2014;72:76-90.
54. Beoy LA et al. Effects of tocotrienol supplementation on hair growth in human volunteers. Tropical life sciences research. Dec 2010;21(2):91-99.
55. Sengupta A et al. Selenoproteins are essential for proper keratinocyte function and skin development. PloS one. 2010;5(8):e12249.
56. Hwang SW et al. Changes in murine hair with dietary selenium excess or deficiency. Experimental dermatology. Apr 2011;20(4):367-369.
57. Razavi M et al. Selenium Supplementation and the Effects on Reproductive Outcomes, Biomarkers of Inflammation, and Oxidative Stress in Women with Polycystic Ovary Syndrome. Hormone and metabolic research. Mar 2016;48(3):185-190.
58. Murugusundram S. Serenoa Repens: Does It have Any Role in the Management of Androgenetic Alopecia? Journal of cutaneous and aesthetic surgery. Jan 2009;2(1):31-32.
59. Prager N et al. A randomized, double-blind, placebo-controlled trial to determine the effectiveness of botanically derived inhibitors of 5-alpha-reductase in the treatment of androgenetic alopecia. Journal of alternative and complementary medicine. Apr 2002;8(2):143-152.
60. Wessagowit V et al. Treatment of male androgenetic alopecia with topical products containing Serenoa repens extract The Australasian journal of dermatology. 2016 Aug;57(3):e76-82.
61. Rossi A et al. Comparitive effectiveness of finasteride vs Serenoa repens in male androgenetic alopecia: a two-year study. International journal of immunopathology and pharmacology. Oct-Dec 2012;25(4):1167-1173.
62. Chittur S et al. Inhibition of inflammatory gene expression in keratinocytes using a composition containing carnitine, thioctic Acid and saw palmetto extract. Evidence-based complementary and alternative medicine: eCAM. 2011;2011:985345.
63. Chen L et al. Blockade of Androgen Markers Using a Novel Betasitosterol, Thioctic Acid and Carnitine-containing Compound in Prostate and Hair Follicle Cell-based Assays. Phytotherapy research. 2016 Jun;30(6):1016-20.
64. Kim YY et al. Effects of topical application of EGCG on testosterone-induced hair loss in a mouse model. Experimental dermatology. Dec 2011;20(12):1015-1017.
65. Esfandiari A et al. The effects of tea polyphenolic compounds on hair loss among rodents. Journal of the National Medical Association. Aug 2005;97(8):1165-1169.
66. Kwon OS et al. Human hair growth enhancement in vitro by green tea epigallocatechin-3-gallate (EGCG). Phytomedicine: international journal of phytotherapy and phytopharmacology. Aug 2007;14(7-8):551-555.
67. Muizzuddin N et al. Beauty from within: Oral administration of a sulfur-containing supplement methylsulfonylmethane improves signs of skin ageing.
68. Guo D et al. Effect of Dietary Methylsulfonylmethane Supplementation on Growth Performance, Hair Quality, Fecal Microbiota, and Metabolome in Ragdoll Kittens. Front Microbiol. 2022 Jul 4;13:838164.
69. Trueb RM. Oxidative stress in ageing of hair. International journal of trichology. Jan 2009;1(1):6-14.
70. Fischer TW et al. Topical melatonin for treatment of androgenetic alopecia. International journal of trichology. Oct 2012;4(4):236-245.
71. Fischer TW et al. Melatonin increases anagen hair rate in women with androgenetic alopecia or diffuse alopecia: results of a pilot randomized controlled trial. Br J Dermatol. Feb 2004;150(2):341-345.
美国脱发病协会
http://www.americanhairloss.org
美国梅奥诊所
www.mayoclinic.org
美国国立斑秃病基金会
http://www.naaf.org
美国医疗在线网
www.webmd.org
加拿大皮肤病网
http://www.dermatology.org
其他参考文献:详见具体的综合干预方案
免责声明和安全信息
英文名称:Alopecia in Women,Hair Thin in Women,
定义
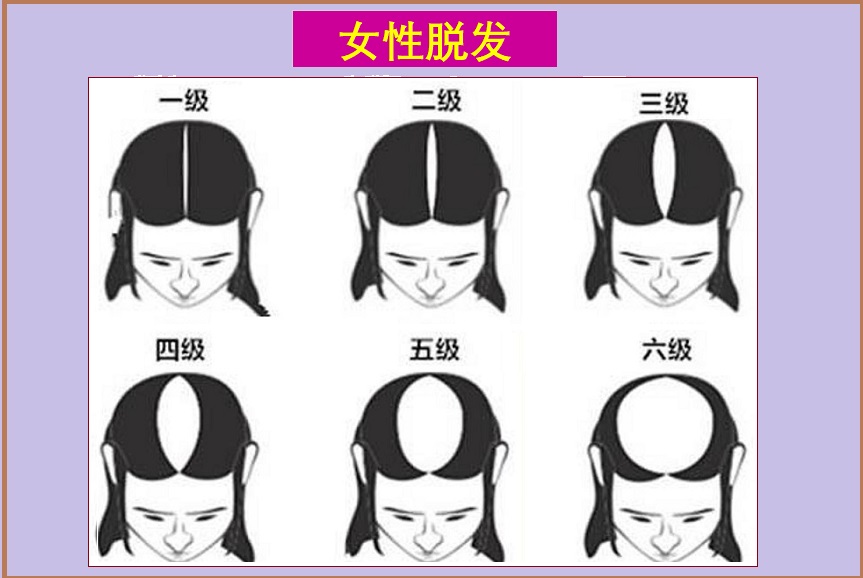
女性脱发通常是指体内雄激素过高等内分泌失调引起的脱发。脱发是指头发脱落的现象,为头发正常生长周期的一部分。如果生长和落发失衡,头发则开始变稀疏、变薄。成人头发大约有10-15万根,绝大部分头发处于生长阶段。但受到年龄、健康状况和其他因素的影响。头发生长周期由以下3个阶段组成:- 生长期(Anagen):头发生长活跃,此阶段头发约占90%,周期2-6年。
- 退化期(Catagen):持续2-3周,毛囊收缩、发根移向头皮表面。
- 休止期(Telogen):约10%处于休止状态,期限2-6个月。休止期结束时,头发脱落,新的毛发从这些毛囊中长出。
- 雄激素性脱发:也分别称为男、女性型脱发(“Pattern” Hair Loss),为最常见的脱发类型,主要与遗传因素、雄激素水平和年龄老化相关。女性主要表现为弥漫性脱发,头顶毛发减少,但不会秃顶。
- 斑秃:在头顶出现圆状斑块,可影响儿童和成年男性和女性,了解更多: 斑秃>>
- 休止期脱发:20-50%头皮毛囊异常过渡到休止期引起脱发增多,主要由心理、生理压力引起,女性比男性更常见。
- 生长期脱发:在生长期的毛发被削弱和破坏,通常由放射治疗和癌症化疗引起,也可能与接触某些有毒物质有关,如重金属等。
- 瘢痕性脱发:通常与潜在的疾病有关,此外,某些发型对头皮的慢性压力、或使用化学药剂也会引起长期的炎症和疤痕。瘢痕性脱发往往是永久性的,常见于30-55岁女性。
- 退化性脱发:随着年龄增长,越来越多毛囊进入休止期,头发自然逐渐变薄、变短,数量减少。大多数女性进入70岁后脱发显著增加。
病因
正常人一般每天损失约100根头发,同时新头发也生长,故一般不会导致头发变薄。当毛发生长和脱落循环被破坏,或毛囊被破坏并被瘢痕组织取代时,就会发生脱发过度或秃头。最常见的雄激素性脱发原因:女性脱发可能由毛囊对双氢睾酮(DHT)的敏感性引起;此外,绝经后雌激素水平下降,也可能有助于脱发。结果导致毛囊逐渐萎缩,以及缩短了头发生长周期,新生头发越来越少。
造成脱发的主要因素可包括如下:
- 遗传或基因因素:影响发病年龄,发病率和脱发程度。
- 激素变化:包括妊娠期、产后和更年期等。
- 健康状况或疾病,包括如下:
- 多囊卵巢综合征,体内雄激素过高,表现为弥漫性脱发。
- 甲状腺功能失调。
- 缺铁性贫血。
- 自体免疫疾病,可引起斑秃。
- 皮肤病,如银屑病、头皮癣、脂溢性皮炎等。
- 肝、肾功能不足。
- 精神创伤,或非常紧张事件。
- 严重的身体创伤。
- 炎症性肠病。
- 重金属中毒等。
- 药物诱导,包括如下:包括
- 口服避孕药。
- 抗甲状腺药物。
- 抗菌和抗病毒药物。
- 抗抑郁药。
- 抗癫痫药物。
- 抗凝血药。
- 化疗和放疗。
- β受体阻滞剂。
- 营养状况不良:
- 严重的蛋白质和必需脂肪酸缺乏。
- 饮食营养不良。
- 铁、锌、生物素和维生素D缺乏症等。
风险因素
以下因素可增加脱发的风险:- 年龄因素,女性绝经后、男性约50岁以上。
- 慢性压力,引起心理、生理变化。
- 营养不足或失衡。
- 一些身体疾病如:
- 自体免疫
- 甲状腺疾病
- 多囊卵巢综合征
- 心血管病
- 代谢综合征
- 前列腺疾病
症状
脱发的症状,包括如下:- 雄激素性脱发:女性主要表现在头顶部,更年期后头发逐渐变得稀薄。
- 斑秃:表现为圆形或卵圆形。
- 瘢痕性脱发:患处皮肤萎缩,毛发不能再生。
疗法
根据不同病因进行治疗,综合疗法包括如下:调整饮食与生活方式
- 健康饮食,包括坚果、蔬菜和水果。
- 限制高脂肪、糖和精加工食品。
- 保证充足、良好睡眠。
- 维持健康体重。
- 学会和运用压力管理,可减少神经性脱发。
营养与草本综合干预
以下是基于循证医学和循证营养学有关文献综合的结果。
有助于防控女性脱发的营养和草药补充剂,主要包括如下:
1.维生素D:
越来越多的证据表明,维生素D参与头发周期的调节1-3。在一个由210名女性型脱发女性组成的案例系列中,超过60%的女性维生素D水平低于正常水平4。血清维生素D水平低与包括斑秃在内的自身免疫性疾病有关5,6。休止期脱发与维生素D缺乏有关7,而维生素D水平低与休止期脱发和女性型脱发女性的脱发程度更高有关8。
在一项为期12周的试验中,48名轻度至中度斑秃患者每天接受二次含有钙泊三醇(维生素D合成形式)的局部溶液治疗。试验结束时,超过62%的参与者的头发再生率达到75%或更好,27%的参与者的发质再生率达到100%9。一名7岁男孩患有斑秃的案例也令人信服:在对局部米诺地尔加氢化可的松没有反应后,该男孩在局部钙泊三醇治疗三个月后经历了完全的头发再生10。一项针对20名斑秃儿童和34名健康对照的研究发现,维生素D水平与脱发严重程度评分呈负相关—随着维生素D水平的升高,脱发严重程度评分下降11。
动物和临床前模型表明,局部使用维生素D和钙泊三醇可能有助于预防化疗诱导的脱发,一些证据表明这种治疗可以促进头发再生12-14。在一项研究中,局部维生素D显著减少了雌性小鼠化疗引起的脱发15。
2.维生素B族:
46名患有弥漫性脱发的妇女每天口服维生素B5 (泛酸)200mg,每天肌肉注射维生素B6,持续20-30天。6个月后重复治疗,结果改善了头发状况,减少了脱发16。动物研究结果表明,维生素B6与L-胱氨酸结合,可防止化疗药物阿霉素引起的脱发17,18。
严重的生物素(维生素B7)缺乏可能是某些基因突变的结果,导致脱发以及其他一些严重的健康问题19。在一项研究中,38%自我报告脱发的女性表现出生物素缺乏症20。在狗身上,补充生物素可能有助于促进毛发生长21,但人类临床试验尚未证实这一发现。一些初步证据表明,补充生物素可能有助于治疗由丙戊酸药物引起的脱发22。
3.角蛋白:
蛋白质缺乏是脱发的一个公认原因,角蛋白是头发的主要成分和主要结构元素。角蛋白合成的年龄相关下降可能导致发干的稳定性和柔韧性恶化23,24。这可能会使头发在梳洗、使用造型产品和工具时容易干燥和断裂。
在一项研究中,在50名有头发紧张或受损迹象的女性中,将一种含有新型可溶性角蛋白(Cynatine®)加维生素和矿物质的补充剂与安慰剂进行了比较。Cynatine含有一种经过特殊处理的、高度生物利用的角蛋白肽形式,是半胱氨酸的丰富来源。90天后,Cynatine配方组的脱发减少,头发强度增加,改善了生长期、休止期和生长期与休止期比率;与安慰剂相比,头发外观更好25。
4.硅:
硅是一种存在于体内的微量元素,被认为是头发的结构成分26。硅化合物在许多可食用植物中很常见27。两项研究着眼于补充提供硅的原硅酸对头发健康的影响。
在一项研究中,50名女性每天服用10mg原硅酸或安慰剂,持续20周。研究结束时,接受硅补充剂的女性头发脆性降低28。在第二项研究中,48名头发细的女性接受了相同的化合物或安慰剂治疗9个月;与安慰剂相比,补充组的头发强度和弹性得到了更好的保留,头发厚度增加29。
5.锌:
锌缺乏与脱发有关30,31。锌在正常毛囊活动、防止毛囊退化和促进毛囊恢复方面发挥着重要作用31。此外,锌可以作为抗雄激素和5-α还原酶的调节剂32。
研究发现,患有雄激素性脱发、休止期脱发和斑秃的男性和女性的血清锌水平都低于没有脱发的人31。早期研究表明,使用锌补充剂纠正相关休止期脱发患者的锌缺乏可以改善脱发33。
斑秃患者锌水平较低与严重程度增加、持续时间延长和治疗耐药性可能性增加有关34,35。在一项非对照临床研究中,15名患有斑秃和低锌水平(≤70mcg/dL)的受试者每天接受50mg葡萄糖酸锌治疗。12周后,9名受试者的头发再生,与锌状况改善相关36。此外,病例报告表明,在接受紫外线加锌治疗的斑秃患者中,持续补充葡萄糖酸锌可能有助于保持头发恢复37。
6.铁:
缺铁会导致休止期脱发38-40。在女性型脱发41,42、休止期脱发42,43和绝经前脱发44的女性中观察到铁蛋白(一种铁储存蛋白)水平较低。一项研究发现,最低的铁蛋白水平与最严重的脱发有关。可以考虑对脱发女性进行铁状况评估,并在必要时补充铁42。
7.必需脂肪酸:
一项针对120名早期脱发女性的试验发现,与对照组相比,六个月内每天补充460mg鱼油、460mg黑加仑籽油(提供γ-亚麻酸GLA)、1mg番茄红素和少量维生素E和维生素C可以改善头发密度。与安慰剂组相比,补充组的生长期头发更多,休止期头发更少45。
在一项啮齿动物研究中,大多数服用DHA(来自鱼油的二十二碳六烯酸)的动物都能免受化疗诱导的脱发的影响46。在另一项针对6只脱发恒河猴的研究中,每天用ω-3(72mg)和ω-6(26mg)脂肪酸治疗与脱发减少有关47。几项研究发现,将DHA与紫杉醇(一种常用的化疗药物)结合,可以减少该药物的毒副作用,包括脱发48-50。
8.生育三烯酚:
生育三烯酚是维生素E家族的成员,天然存在于大麦、小麦胚芽以及某些类型的谷物和坚果中51。与更常见的维生素E形式生育酚类似,有四种生育三烯酚标记为α、β、γ和δ51,52。生育三烯酚被认为具有重要的维生素E活性,特别是在抗炎、降低胆固醇和辐射防护方面52,53。
新出现的证据表明,生育三烯酚可能有助于促进头发健康。在一项涉及38名患有不同类型和程度脱发的女性和男性的研究中,接受23IUα-生育酚加50mg混合生育三烯醇补充剂的患者在八个月内头发数量增加了34%以上,而接受安慰剂的患者头发数量略有减少54。
9.硒:
硒的摄入对健康的毛囊功能很重要,硒缺乏可能在脱发中发挥作用55,56。在一项针对64名多囊卵巢综合征女性的为期八周的随机对照试验中,32名女性每天补充200mcg硒,另一半女性则服用安慰剂。试验结束时,与安慰剂相比,硒组的脱发显著减少57。
10.锯棕榈:
锯棕榈被广泛用于治疗前列腺肥大和雄激素性脱发58。一项针对26名23-64岁、患有轻至中度雄激素性脱发男性的随机对照试验发现,200mg锯棕榈提取物、50mg β-谷甾醇以及补充量的卵磷脂、胆碱、肌醇、烟酸和生物素的组合,对头发生长和质量测量是有效的。对头发生长和外观满意度的自我评估,以及研究者对头发密度的评估都显著改善59。
一项针对50名20至50岁雄激素性脱发男性的非对照研究发现,局部使用锯棕榈会增加头发数量60。另一项试验对100名轻度至中度雄激素性脱发患者进行了为期两年的每日320mg锯叶棕榈提取物和每日1mg非那雄胺的疗效比较。非那雄胺使68%的受试者的头发再生,而锯棕榈组中38%的受试人的头发生长得到改善;锯棕榈的治疗耐受性良好61。研究人员认为,锯棕榈抑制5-α还原酶的能力至少是其积极作用的部分原因58;一些人提出,将锯棕榈或β-谷甾醇与肉碱和α-硫辛酸等抗炎剂结合可能会增强其有效性62,63。
11.绿茶:
有证据表明,绿茶及其主要多酚表没食子儿茶素没食子酸盐(EGCG)可能有助于防止脱发和帮助头发再生。在一项小鼠研究中,局部EGCG溶液可防止睾酮诱导的脱发64。在一项针对自发性脱发小鼠的研究中,添加到饮用水中的绿茶多酚溶液促进了头发的生长,而不是用白开水促进头发的生长65。EGCG在实验室环境中以及在人类受试者中刺激真皮乳头细胞并促进人类毛囊中的毛发生长66。
12.甲磺酰甲烷(MSM):
一种天然含硫有机物质,具有抗氧化、抗炎、抗皮肤衰老和促进头发生长等多种生物功能67,68。动物研究表明,饮食中补充0.2%的MSM可以改善小猫的毛发质量68。
13.褪黑素(外用):
褪黑激素可能有助于脱发的局部治疗。虽然还不知道褪黑素是如何对抗脱发的,但它对抗氧化应激的能力,被认为在脱发中起着重要作用69,以及它刺激毛囊生长的能力已经被提出70。
在一项早期对照试验中,40名患有女性脱发或弥漫性脱发的女性每晚在头部涂抹1毫升0.1%的局部褪黑素溶液或安慰剂溶液。六个月后,局部褪黑素组在生长期的头发明显增多71。
一组针对早期雄激素性脱发男性和女性的四项研究评估了褪黑素与其他外用药物联合治疗脱发的效果。在第一项研究中,将同样含有生物素和银杏叶提取物的0.0033%褪黑素溶液每晚涂抹在30名男性和女性的头皮上,持续90天。研究人员和参与者都报告说,脱发的严重程度在第30天有所下降,在第90天有了更大的改善。在第二项研究中,35名男性在六个月内每晚使用相同的溶液。研究人员注意到,三个月后头发数量和密度平均增加了29%,六个月后数量和密度分别增加了近43%和41%,超过50%的参与者对治疗有反应。第三项研究使用了毛发计数测试,参与者计算每天早上梳头60秒时脱落的毛发数量,作为衡量反应的指标。在为期90天的试验中,20名女性参与者的脱发数量有所下降,但使用褪黑素溶液的40名男性参与者的脱发量没有下降。最后一项研究包括901名男性和990名女性,他们每晚使用该溶液。拔毛测试显示,经过90天的治疗,近62%的参与者没有脱发,近23%的参与者有新的头发生长。此外,褪黑素溶液治疗似乎可以改善患有这种头皮疾病的参与者的脂溢(红色、发痒、鳞状皮肤)70。
更多内容可点击其个性化综合干预方案如下:
- 头发健康管理:
- 营养护法:
- 弥漫性脱发管理:
- 女性神经性脱发管理:
- 缺铁性脱发管理:
以及参阅本网如下专文了解更多:
医疗干预
如果脱发由疾病引起,通过治疗、身体康复后头发会重新长出。
医生可能推荐如下治疗措施:
- 雄激素性脱发:米诺地尔酊外擦。
- 休止期脱发:主要由身体或心理压力引起,通常在脱发开始前2-4个月就存在。压力消除后,4-6个月内头发一般会再生。如果压力反复或慢性压力,脱发持续发生,医生可能建议局部使用米诺地尔酊剂。
- 生长期脱发:头皮冷却治疗。
- 植发:头皮毛发种植术也可作为选项。
预防
大多数脱发是由遗传(女性型脱发)引起的,这种类型脱发是不可预防的。有助于预防一些脱发的措施包括如下:
- 化学性脱发,不使用刺激性强的染发剂、烫发剂及劣质洗发用品。
- 物理性脱发,不要使用易产生静电的塑料梳子和塑料头刷,在空气粉尘污染严重的环境戴防护帽并及时洗头。
- 营养性脱发应加强营养,多吃蔬果、海带、核桃仁等。
- 脂溢性脱发要少吃油腻重的食物,加强运动锻炼。
- 避免发型过紧,如扎辫子、马尾辫。
- 避免强迫扭曲,如摩擦或拉扯头发。
- 洗涤和刷牙时,请轻轻抚摸头发。
- 用宽齿梳头为宜。
- 限制使用苛刻的处理方法,如热辊、烫发器和热油处理等。
- 避免可能导致脱发的药物。
- 保护头发免受阳光和其他紫外线的伤害。
参考文献:
1. Amor KT et al. Does D matter? The role of vitamin D in hair disorders and hair follicle cycling. Dermatology online journal. 2010;16(2):3.
2. Malloy PJ et al. The role of vitamin D receptor mutations in the development of alopecia. Molecular and cellular endocrinology. Dec 5 2011;347(1-2):90-96.
3. Aoi N et al. 1alpha,25-dihydroxyvitamin D3 modulates the hair-inductive capacity of dermal papilla cells: therapeutic potential for hair regeneration. Stem cells translational medicine. Aug 2012;1(8):615-626.
4. Siah TW et al. Female Pattern Hair Loss: A Retrospective Study in a Tertiary Referral Center. International journal of trichology. Apr-Jun 2016;8(2):57-61.
5. Mahamid M et al. Association between vitamin D levels and alopecia areata. The Israel Medical Association journal: IMAJ. Jun 2014;16(6):367-370.
6. Aksu Cerman A et al. Vitamin D deficiency in alopecia areata. Br J Dermatol. Jun 2014;170(6):1299-1304.
7. Cheung EJ et al. Vitamin and Mineral Deficiencies in Patients With Telogen Effluvium: A Retrospective Cross-Sectional Study. Journal of drugs in dermatology. Oct 01 2016;15(10):1235-1237.
8. Rasheed H et al. Serum ferritin and vitamin d in female hair loss: do they play a role? Skin Pharmacol Physiol. 2013;26(2):101-107.
9. Cerman AA et al. Topical Calcipotriol Therapy for Mild-to-Moderate Alopecia Areata: A Retrospective Study. J Drugs Dermatol. Jun 2015;14(6):616-620.
10. Kim DH et al. Successful treatment of alopecia areata with topical calcipotriol. Annals of dermatology. Aug 2012;24(3):341-344.
11. Unal M et al. Serum vitamin D level is related to disease severity in pediatric alopecia areata. Journal of cosmetic dermatology. Apr 26 2017.
12. Jimenez JJ et al. Protection from chemotherapy-induced alopecia by 1,25-dihydroxyvitamin D3. Cancer research. Sep 15 1992;52(18):5123-5125.
13. Schilli MB et al. Reduction of intrafollicular apoptosis in chemotherapy-induced alopecia by topical calcitriol-analogs. The Journal of investigative dermatology. Oct 1998;111(4):598-604.
14. Wang J et al. Protection against chemotherapy-induced alopecia. Pharmaceutical research. Nov 2006;23(11):2505-2514.
15. Chen G et al. Protection against cyclophosphamide-induced alopecia and inhibition of mammary tumor growth by topical 1,25-dihydroxyvitamin D3 in mice. International journal of cancer. Jan 19 1998;75(2):303-309.
16. Brzezinska-Wcislo L. [Evaluation of vitamin B6 and calcium pantothenate effectiveness on hair growth from clinical and trichographic aspects for treatment of diffuse alopecia in women]. Wiadomosci lekarskie (Warsaw, Poland: 1960). 2001;54(1-2):11-18.
17. D'Agostini F et al. Chemoprevention of doxorubicin-induced alopecia in mice by dietary administration of L-cystine and vitamin B6. Archives of dermatological research. Jan 2013;305(1):25-34.
18. D'Agostini F et al Chemoprevention of smoke-induced alopecia in mice by oral administration of L-cystine and vitamin B6. J Dermatol Sci. Jun 2007;46(3):189-198.
19. Zempleni J et al. Biotin and biotinidase deficiency. Expert review of endocrinology & metabolism. 2008;3(6):715-724.
20. Trueb RM. Serum Biotin Levels in Women Complaining of Hair Loss. International journal of trichology. Apr-Jun 2016;8(2):73-77.
21. Frigg M et al. Clinical study on the effect of biotin on skin conditions in dogs. Schweizer Archiv fur Tierheilkunde. 1989;131(10):621-625.
22. Famenini S et al. Evidence for supplemental treatments in androgenetic alopecia. J Drugs Dermatol. Jul 2014;13(7):809-812.
23. Giesen M et al. Ageing processes influence keratin and KAP expression in human hair follicles. Experimental dermatology. Sep 2011;20(9):759-761.
24. Mubki T et al. Evaluation and diagnosis of the hair loss patient: part II. Trichoscopic and laboratory evaluations. Journal of the American Academy of Dermatology. Sep 2014b;71(3):431.e431-431.e411.
25. Beer C et al. A clinical trial to investigate the effect of Cynatine HNS on hair and nail parameters. TheScientificWorldJournal. 2014;2014:641723.
26. Martin KR. Silicon: the health benefits of a metalloid. Metal ions in life sciences. 2013;13:451-473.
27. Jurkic LM et al. Biological and therapeutic effects of ortho-silicic acid and some ortho-silicic acid-releasing compounds: New perspectives for therapy. Nutrition & metabolism. 2013;10(1):2.
28. Barel A et al. Effect of oral intake of choline-stabilized orthosilicic acid on skin, nails and hair in women with photodamaged skin. Archives of dermatological research. Oct 2005;297(4):147-153.
29. Wickett RR et al. Effect of oral intake of choline-stabilized orthosilicic acid on hair tensile strength and morphology in women with fine hair. Archives of dermatological research. Dec 2007;299(10):499-505.
30. Saper RB et al. Zinc: an essential micronutrient. American family physician. May 1 2009;79(9):768-772.
31. Kil MS et al. Analysis of serum zinc and copper concentrations in hair loss. Annals of dermatology. Nov 2013;25(4):405-409.
32. Gupta M et al. Zinc therapy in dermatology: a review. Dermatol Res Pract. 2014;2014:709152.
33. Karashima T et al. Oral zinc therapy for zinc deficiency-related telogen effluvium. Dermatologic therapy. Mar-Apr 2012;25(2):210-213.
34. Abdel Fattah NS et al. Evaluation of serum zinc level in patients with newly diagnosed and resistant alopecia areata. Int J Dermatol. Jan 2016;55(1):24-29.
35. Bhat YJ et al. Trace element levels in alopecia areata. Indian journal of dermatology, venereology and leprology. Jan-Feb 2009;75(1):29-31.
36. Park H et al. The therapeutic effect and the changed serum zinc level after zinc supplementation in alopecia areata patients who had a low serum zinc level. Annals of dermatology. May 2009;21(2):142-146.
37. Lux-Battistelli C. Combination therapy with zinc gluconate and PUVA for alopecia areata totalis: an adjunctive but crucial role of zinc supplementation. Dermatologic therapy. Jul-Aug 2015;28(4):235-238.
38. Grover C et al. Telogen effluvium. Indian journal of dermatology, venereology and leprology. Sep-Oct 2013;79(5):591-603.
39. Levy LL et al. Female pattern alopecia: current perspectives. International journal of women's health. 2013;5:541-556.
40. Malkud S. Telogen Effluvium: A Review. Journal of clinical and diagnostic research: JCDR. Sep 2015;9(9):We01-03.
41. Park SY et al. Iron plays a certain role in patterned hair loss. J Korean Med Sci. Jun 2013;28(6):934-938.
42. Rasheed H et al. Serum ferritin and vitamin d in female hair loss: do they play a role? Skin Pharmacol Physiol. 2013;26(2):101-107.
43. Moeinvaziri M et al. Iron status in diffuse telogen hair loss among women. Acta dermatovenerologica Croatica: ADC. 2009;17(4):279-284.
44. Deloche C et al. Low iron stores: a risk factor for excessive hair loss in non-menopausal women. European journal of dermatology: EJD. Nov-Dec 2007;17(6):507-512.
45. Le Floc'h C et al. Effect of a nutritional supplement on hair loss in women. Journal of cosmetic dermatology. Mar 2015;14(1):76-82.
46. Takahata K et al. Protection from chemotherapy-induced alopecia by docosahexaenoic acid. Lipids. 1999;34 Suppl:S105.
47. Hamel AF et al. Fatty acid supplements improve hair coat condition in rhesus macaques. Journal of medical primatology. 2017 Oct;46(5):248-251.
48. Bradley MO et al. Tumor targeting by conjugation of DHA to paclitaxel. Journal of controlled release: official journal of the Controlled Release Society. Jul 6 2001;74(1-3):233-236.
49. Wolff AC et al. Phase I study of docosahexaenoic acid-paclitaxel: a taxane-fatty acid conjugate with a unique pharmacology and toxicity profile. Clinical cancer research. Sep 1 2003;9(10 Pt 1):3589-3597.
50. Harries M et al. Phase I/II study of DHA-paclitaxel in combination with carboplatin in patients with advanced malignant solid tumours. British journal of cancer. Nov 1 2004;91(9):1651-1655.
51. Ahsan H et al. A review of characterization of tocotrienols from plant oils and foods. J Chem Biol. 2015;8(2):45-59.
52. Peh HY et al. Vitamin E therapy beyond cancer: Tocopherol versus tocotrienol. Pharmacol Ther. 2016;162:152-169.
53. Jiang Q. Natural forms of vitamin E: metabolism, antioxidant, and anti-inflammatory activities and their role in disease prevention and therapy. Free Radic Biol Med. 2014;72:76-90.
54. Beoy LA et al. Effects of tocotrienol supplementation on hair growth in human volunteers. Tropical life sciences research. Dec 2010;21(2):91-99.
55. Sengupta A et al. Selenoproteins are essential for proper keratinocyte function and skin development. PloS one. 2010;5(8):e12249.
56. Hwang SW et al. Changes in murine hair with dietary selenium excess or deficiency. Experimental dermatology. Apr 2011;20(4):367-369.
57. Razavi M et al. Selenium Supplementation and the Effects on Reproductive Outcomes, Biomarkers of Inflammation, and Oxidative Stress in Women with Polycystic Ovary Syndrome. Hormone and metabolic research. Mar 2016;48(3):185-190.
58. Murugusundram S. Serenoa Repens: Does It have Any Role in the Management of Androgenetic Alopecia? Journal of cutaneous and aesthetic surgery. Jan 2009;2(1):31-32.
59. Prager N et al. A randomized, double-blind, placebo-controlled trial to determine the effectiveness of botanically derived inhibitors of 5-alpha-reductase in the treatment of androgenetic alopecia. Journal of alternative and complementary medicine. Apr 2002;8(2):143-152.
60. Wessagowit V et al. Treatment of male androgenetic alopecia with topical products containing Serenoa repens extract The Australasian journal of dermatology. 2016 Aug;57(3):e76-82.
61. Rossi A et al. Comparitive effectiveness of finasteride vs Serenoa repens in male androgenetic alopecia: a two-year study. International journal of immunopathology and pharmacology. Oct-Dec 2012;25(4):1167-1173.
62. Chittur S et al. Inhibition of inflammatory gene expression in keratinocytes using a composition containing carnitine, thioctic Acid and saw palmetto extract. Evidence-based complementary and alternative medicine: eCAM. 2011;2011:985345.
63. Chen L et al. Blockade of Androgen Markers Using a Novel Betasitosterol, Thioctic Acid and Carnitine-containing Compound in Prostate and Hair Follicle Cell-based Assays. Phytotherapy research. 2016 Jun;30(6):1016-20.
64. Kim YY et al. Effects of topical application of EGCG on testosterone-induced hair loss in a mouse model. Experimental dermatology. Dec 2011;20(12):1015-1017.
65. Esfandiari A et al. The effects of tea polyphenolic compounds on hair loss among rodents. Journal of the National Medical Association. Aug 2005;97(8):1165-1169.
66. Kwon OS et al. Human hair growth enhancement in vitro by green tea epigallocatechin-3-gallate (EGCG). Phytomedicine: international journal of phytotherapy and phytopharmacology. Aug 2007;14(7-8):551-555.
67. Muizzuddin N et al. Beauty from within: Oral administration of a sulfur-containing supplement methylsulfonylmethane improves signs of skin ageing.
68. Guo D et al. Effect of Dietary Methylsulfonylmethane Supplementation on Growth Performance, Hair Quality, Fecal Microbiota, and Metabolome in Ragdoll Kittens. Front Microbiol. 2022 Jul 4;13:838164.
69. Trueb RM. Oxidative stress in ageing of hair. International journal of trichology. Jan 2009;1(1):6-14.
70. Fischer TW et al. Topical melatonin for treatment of androgenetic alopecia. International journal of trichology. Oct 2012;4(4):236-245.
71. Fischer TW et al. Melatonin increases anagen hair rate in women with androgenetic alopecia or diffuse alopecia: results of a pilot randomized controlled trial. Br J Dermatol. Feb 2004;150(2):341-345.
参考来源:
美国脱发病协会
http://www.americanhairloss.org
美国梅奥诊所
www.mayoclinic.org
美国国立斑秃病基金会
http://www.naaf.org
美国医疗在线网
www.webmd.org
加拿大皮肤病网
http://www.dermatology.org
其他参考文献:详见具体的综合干预方案
免责声明和安全信息
- 本信息(包括任何附带资料)不是为了取代医生或有关合格从业人士的建议或忠告。
- 任何人如果想要对本文涉及的药物、饮食、运动或其他生活方式的使用、或改变调整,以预防或治疗某一特定健康状况或疾病,应首先咨询医生或有关合格从业人士,并获得他/她们的许可。妊娠和哺乳妇女在使用本网站任何内容前,尤其应征求医生的意见。
- 除非另有说明,本网站所述内容仅适用于成人。
- 本网站所推荐的任何产品,消费者应该以实际的产品标签内容为准,尤其应关注重要的安全信息以及产品最新信息,包括剂量、使用方法和禁忌症等。
- 由于循证医学研究、文献及有关产品处于不断的变化中,本网站工作人员将尽力更新。
- 本网站不能保证所载文章内容、综合干预方案以及相关成分或产品述及的健康益处,也不承担任何责任。